

When Nora suffered a lifechanging incident requiring an ITU stay, she was left unable to verbally communicate her needs or wishes. She was admitted to The Bridge Neurological Care Centre with a cuffed tracheostomy tube and required ventilation, where she began speech and language therapy. This is the inspiring story of her rehabilitation journey to regain her ability to communicate and enjoy eating and drinking again.
Metabolic encephalopathy with severe motor sensory axonal neuropathy
When Nora was admitted to The Bridge Neurological Care Centre in November 2021, she had weakness in all four limbs and reduced trunk and head control. On admission, Nora had a cuffed tracheostomy tube (a tube that has an inflatable balloon-like inserted into the windpipe in an opening created at the front of the neck to help you breathe) and required ventilation. She was unable to communicate any of her needs verbally with very restricted non-verbal communication due to her physical presentation.
Nora had suffered a metabolic encephalopathy with severe motor sensory axonal neuropathy which had required an ITU stay. Metabolic encephalopathy is defined as an alteration in consciousness caused by diffuse or global brain dysfunction from impaired cerebral metabolism (J. Claude Hemphill, 2021). Axonal neuropathy is a condition in which the nerve cells begin to function abnormally because the axons (a thin fibre that extends from a nerve cell) are degenerating, affecting Nora’s sensory perception and movement.
Unable to eat or drink orally, all of Nora’s nutrition, hydration and medication needs were met via a Nasogastric Tube (a thin tube passed through the nose and into the stomach). The NG had been replaced later with a P.E.G (a small tube that is inserted through the skin directly in to the stomach to administer feed, fluid and medication without swallowing).
Speech and Language Therapy
When Nora was first assessed by the Speech and Language Therapy (SALT) team, she was noted to have infrequent spontaneous saliva swallow and weak muscles affecting her eating/drinking abilities and swallow safety. She was communicating using head movements for yes/ no and using a letter board to spell out what she wished to communicate. However, this was effortful and frustrating for Nora as she wanted to communicate faster and easier.
Her SALT assessment also included written language and AAC (Alternative and Augmentative Communication) evaluation to explore and implement all possible means of communication. Mira Bou Akar, Lead Speech and Language Therapist at The Bridge Neurological Care Centre, explains why using the AAC and exploring all possible means of communication was so important.
Mira says: “Not being able to speak is very distressing. Normally our speech is very spontaneous, we don’t have to think about how or when we do it, and we are not consciously putting effort into it. But when we lose the ability to speak and communicate it impacts our wellbeing and everything we do in our life. That’s why it was so important to explore all possible communications methods with Nora to give her the best opportunity to express herself.”
The SALT team at The Bridge began a comprehensive therapy program that involved exploring and installing varied AAC means to facilitate communication. This intervention included going through questionnaires, formal and informal meetings with Nora, her family and staff members to tailor AAC resources according to her individual needs.
The SALT, along with the OT team coordinated with the Regional Communication Aids and Environmental Control Services to install a communication and environmental control device. Varied access methods were explored including eye-gaze and head switch. Mira Bou Akar, Lead Speech and Language Therapist also liaised with an international USA-Australian based company to arrange for a high-tech device trial to explore EMG switch suitability (EMG enables communication through electrodes placed on the skin, detecting minimal muscles twitches). Swallowing rehabilitation focused on improving oral and pharyngeal muscular strength and range of movement with limited oral trials of coated spoons of water to maintain swallow function.
Rehab milestones
Following her progression with physiotherapy, Nora managed to have an un-cuffed tracheostomy tube inserted in January 2022. This was a turning point in Nora’s journey as she was able to vocalise and progress further with her swallowing rehabilitation. Nora’s speech was non-intelligible at this point due to poor breath support, poor phonation and breathing/ speech coordination, inaccurate articulation and weak muscles. Verbal communication and swallowing were still challenging.
An intensive verbal communication, voice and swallowing rehabilitation program was formulated following Nora’s progression. This program focused on improving the muscles involved in swallowing with varied manoeuvres and exercises, progressively increasing oral trials amounts and frequency while safely exploring varied consistencies.
The program also aimed to improve vocal quality, breath support so Nora could communicate using sentences rather than single words, speech intelligibility and articulation accuracy. In February 2022, Nora was communicating her basic needs verbally using two word sentences, not needing her AAC device.
As Mira Bou Akar explains this was an incredible achievement for Nora:
“It was very exciting for Nora because before when she was using AAC it was so hard for her. For example, when she used a letterboard, she had to spell every single word, which was exhausting. The picture board was also particularly tiring, plus the boards, even at their best, are limited in what you can communicate through them. What you manage to communicate is not accurate to what you actually want to say, there’s lots of words missing, for example.
“So when Nora was able to use two word sentences it was really good for both for her and the team because we were able to understand her needs a lot quicker, a lot easier. She was really happy being able to communicate again and it improved her wellbeing because she saw progression.”
A year later
Nora continued to improve and a year later, Nora was communicating verbally with intelligible speech, good vocal loudness and using long, complex sentences. She managed, with support from the physiotherapy and nursing team, to be successfully weaned off ventilation and was decannulated (tracheostomy tube removed). Respiratory Muscle Strength Training (RMST) was introduced in SALT to further support her voice and swallowing outcomes.
Regular swallowing re-assessments were conducted with ongoing increased amounts of oral intake during speech and language therapy sessions while closely liaising with the multidisciplinary team to ensure chest health was maintained. SALT assisted in training staff members in dysphagia (swallowing difficulties) and progressively handed-over oral trials to dysphagia trained members during daily mealtime supervised sessions.
Mira Bou Akar explains why training on the communication and comprehension abilities of individuals is essential to provide effective care.
Mira says: “It’s very important to train team members on the comprehension level the individual has so we provide appropriate communication support rather than abruptly interrupting the communication process or not allowing enough time to process information and then respond. Without proper training we could give another instruction, or an explanation too quickly – this is not helpful and ultimately confuses and frustrates the individual.
“We need to adapt the way we speak so that it fits an individual’s cognitive abilities. Some of the residents might not understand long sentences. They would need information to be broken down and given as simple words, simple phrases, otherwise the communication will not be successful.
“For example, the individual might have memory difficulties or cognitive difficulties, so we need to adapt our approach. If a team member is going through the menu at lunchtime, rather than reading the whole menu then asking them what they want, we would take it in chunks. Team members are trained to break things down to support with cognitive issues.
“Also a lot of people we support at The Bridge have difficulties seeing the full visual field, so they might only be able to see part of the visual field. This has implications when using AAC, for example, where we present the cards so they can see them.”

Progression with eating and drinking
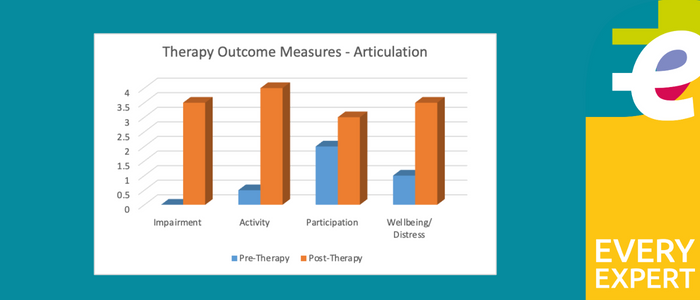
In March 2023, Nora started eating and drinking modified consistencies again and kept progressing nicely with her swallowing, achieving a soft and bite-sized diet. Nora depended less and less on her PEG for nutrition and hydration until she was no longer requiring any PEG feed. Nora’s likes and dislikes were fed-back to the catering team to ensure mealtimes were as enjoyable as possible while varying the taste stimulation as part of the swallowing program. In coordination with the dietitian, Nora’s PEG feed was being reduced progressively as her oral intake has been increasing. The following outcomes charts illustrate Nora’s progress following therapy.
Mira shares how inspiring Nora’s journey has been both for herself and the whole team.
“Nora has progressed from not being able to speak to being completely dependent on her verbal communication to a point where she does not need any communication aids. She has given her communications device back because she doesn’t need it.
“At the beginning, she would have all her feed through a tube via her nose, into her stomach as she couldn’t eat. When she was discharged she was eating a consistency that required even chewing, she was having proper food and I know that she will continue to progress, hopefully to a normal diet soon.
“Nora has done amazingly well and is an incredible inspiration to us all. She was in tears of joy and excitement when she first started eating and drinking again and regained her speech. It is moments like these that make speech and language therapy and multidisciplinary neurorehabilitation so rewarding!”
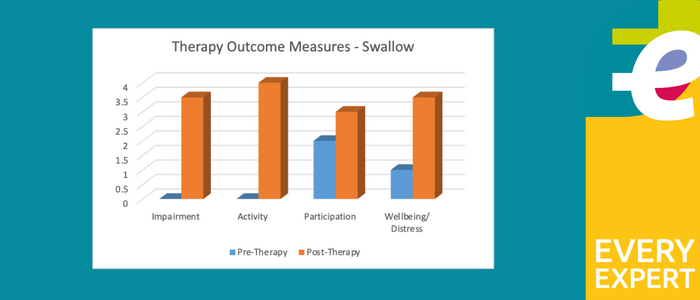
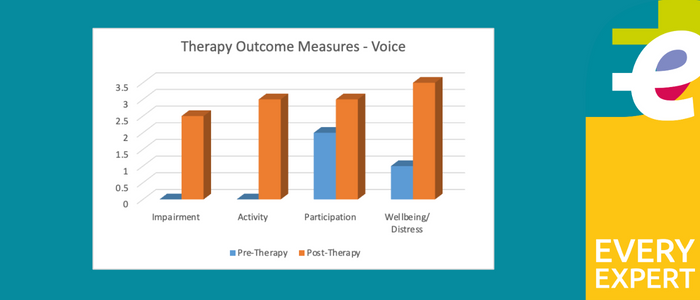
Therapy outcome measures
The images below show the Therapy Outcome Measures for Pre-Therapy and Post-Therapy for swallow, voice, and articulation.
References:
Claude Hemphill J. (2021). Disorders of Consciousness in Systematic Diseases. Aminoff’s Neurology and General Medicine (Sixth Edition). Science Direct. URL: https://www.sciencedirect.com/topics/medicine-and-dentistry/metabolic-encephalopathy
Make An Enquiry
If you’d like to make a referral then please get in touch with us.
You can also visit each service’s profile page to find out more about what our EveryExpert approach to care looks like in practice:
Adderley Green, Staffordshire
Badby Park, Northamptonshire
Garden & Jacobs, Hertfordshire
St Neots, Cambridgeshire
Stanley House, Herefordshire
The Avalon Centre, Wiltshire
The Bridge, Middlesbrough, Wiltshire
The Dean, Gloucestershire
