


How psychology can help problem-solving: a training case example on a medium secure ward
by Sarah Lund
Forensic Psychologist in Training, Thornford Park Hospital
How psychology can help with problem-solving
One of the key roles undertaken by psychologists in multi-disciplinary teams is the provision of psychological information to help the team to solve problems. Whilst this is central to the psychologist’s role, many healthcare staff are often more familiar with the psychologist’s role in working directly with service users (Wood, Williams, Billings & Johnson, 2019).
As members of a multi-disciplinary team, the aim of the psychologist is not to solve the problem for the team, but to provide the team with the information they need to solve the problem themselves (Ireland, 2010). Psychologists do this by using their knowledge of human behaviour and thinking processes to guide the team in effective decision-making and problem-solving.
Before any advice can be given, the problem must be clearly understood. It may be the case that the team have already identified the problem to be advised on, or alternatively, the psychologist can help the team to define the problem. Once the problem is clear, psychologists can work with the team to identify how the problem can be solved. This might be done by sharing information in written reports, giving verbal feedback in MDT or CPA meetings, or through supervision and reflective practice. Psychologists may then have a role in implementing and evaluating the chosen solution.
A training case example on a medium secure ward
The following case example demonstrates how the ward psychologist used training to resolve difficulties relating to boundaries on a medium secure ward.
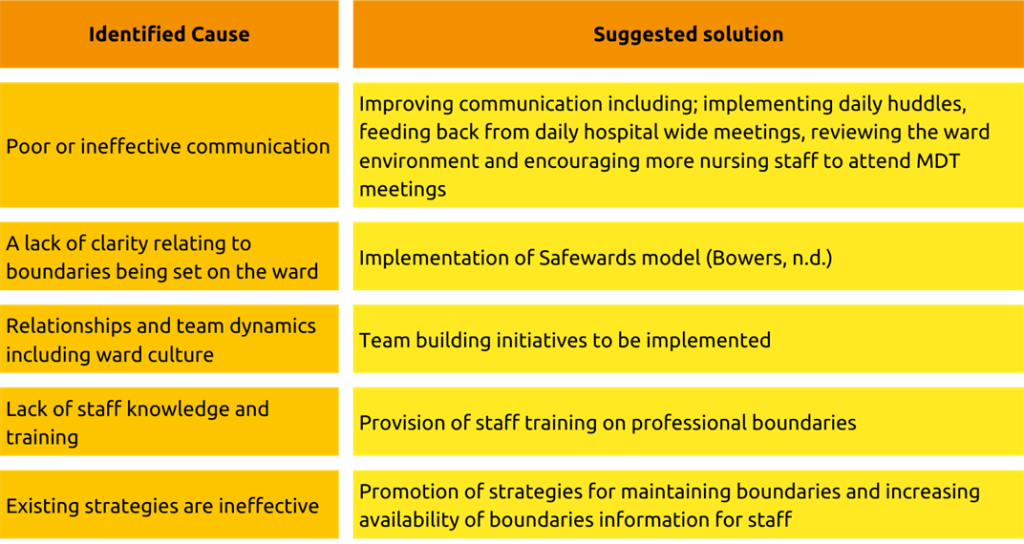
Defining the problem – Through MDT discussions, it was noted that there was a higher-than-expected number of boundary breaches occurring on the ward. This was recognised as a potential threat to the safety of the ward environment, the service users and the staff (Adshead, 2012). In order to understand the types of boundary breaches that were happening, and why they were happening, the team agreed for the ward psychologist to investigate. Nursing and other multi-disciplinary staff were interviewed to gather information on the extent and causes of the problem. Through the interview process, a number of causes for boundary breaches were identified and matched with possible solutions. The causes and suggested solutions are shown in Table 1, below. These were presented to the team in a written report that outlined the advantages of each solution, allowing the team to make an informed decision.
Designing the training – Once the team had agreed for training to be provided to staff, the training was designed using information gained from the interviews with the team. The training focused on developing staff knowledge of what boundary breaches are, and why they occur. This included consideration of service user factors, as well as staff and organisational factors (Adshead, 2012). Principles of effective learning were followed to maximise the impact of the training.
Delivering the training – The training was delivered to as many members of the team as possible, with four face-to-face training sessions offered across two days. By providing the training face-to-face, staff were able to share experiences and discuss issues in-depth. Real-life examples were discussed, enabling staff to plan together how to use the training with the service users on the ward. After the training, the ward psychologist provided staff with on-the-job support to apply their learning on the ward.
Evaluating the training – A thorough evaluation of the training was completed. The staff response to the training was overwhelmingly positive and the majority of staff asked for further, or more regular, boundary training. Evaluation over the months following the training included monitoring of how staff were using their learning from the training on the ward through discussions with staff and incident reporting. This evaluation found that, after the training, staff had a better understanding of what is expected from them in terms of boundaries and they were better able to identify when breaches were occurring.
You can learn more about Thornford Park Hospital on the service page.
References:
Adshead, G. (2012) What the eye doesn’t see: relationships, boundaries, and forensic mental health. In A. Aiyegbusi & G. Kelly (Eds.) Professional and Therapeutic Boundaries in Forensic Mental Health Practice (pp. 13-32).
Bowers, L. (n.d.) Safewards: A new model of conflict and containment on psychiatric wards.
Ireland, C. A. (2010) The Role of a Consultant: Function, skills competences and presentation. In C. A. Ireland & M. J. Fisher (Eds) Consultancy and Advising in Forensic Practice: Empirical and Practical Guidelines (pp3-16). Chichester, England: BPS Blackwell.
Wood, L., Williams, C., Billings, J., & Johnson, S. (2019) The role of psychology in a multidisciplinary psychiatric inpatient setting: Perspective from the multidisciplinary team. Psychology and Psychotherapy: Theory, Research and Practice, 92, 554-564. doi: 10.1111/papt.12199