

Communication is more than just what we say. According to Mehrabian’s Communication Model (1971), only 7% of our communication is verbal and 93% is non-verbal. Most of our predictions and inferences used within communication are based on a person’s non-verbal behaviour, using body language, facial expressions or tone of voice. Individuals with acquired brain injury or cognitive decline often struggle to understand non-verbal cues which can result in socially inappropriate behaviour and make living within the community a challenge.
The Avalon Centre in Wiltshire is a neurobehavioural centre for men and women who have an acquired brain injury. The centre has been designed specifically to support people who, because of their injury, have challenging and complex needs and benefit from a neurobehavioural approach to their rehabilitation. The Avalon Centre operates a transdisciplinary team (TDT) model, which is considered a cornerstone of neurobehavioural rehabilitation. TDT requires all members of the team to be familiar with each patient’s person centred goals, enabling the opportunity for rehabilitation across the day in all settings.
Angela Kavanagh is Specialist Speech & Language Therapist (SLT) & Therapy Lead at the Avalon Centre and specialises in working with adults who have complex communication and swallowing difficulties as result of an acquired brain injury. Angela recently completed training on the assessment and intervention of social skills. Her learning has enabled her to implement a successful social communication intervention with an individual which has dramatically reduced socially inappropriate behaviour and helped achieve important rehabilitation goals. In this EveryExpert article we chat with Angela about these interventions and the importance of the TDT for transferring the outcomes into daily life and a community setting.

Great to talk with you Angela, could you start by telling me about the training that you completed?
“I attended a three-day ‘Talkabout’ course on assessing and teaching social skills, authored by Alex Kelly. The course explored not only social communication skills, but the importance of self-awareness and the awareness of others. These are skills that influence the ability to establish effective and healthy relationships and shape the decisions that we make. I learnt how to assess self-awareness and self-esteem and the importance in a TDT approach to the assessment of social skills.”
Can you explain how you used your new learning to implement a successful social communication intervention?
“Of course. The individual I supported is ER, a man in his late 30s who suffered an aneurysm, secondary to chronic hypertension, in 2023. He was referred to the Avalon Centre from the Acute Neurosciences inpatient setting in the John Radcliffe Hospital, for neurobehavioural rehabilitation and to assess the impact of the brain injury on his functioning, including factors that may affect his ability to be safely discharged home to his family. For the first three months following admission, initial assessments and observations were completed by the TDT. When I completed my initial communication and language assessments I was not alerted to any serious concerns with regards to speech or language impairment.
“However during the first CPA meeting, the wider TDT reflected on the severity of the socially inappropriate behaviours that ER was displaying. For example, he had very poor social distancing and often invaded the personal space of staff and patients. He was unable to sit still and was constantly pacing around the ward and fidgeting. Due to the nature of the inappropriate comments directed towards female members of staff all interactions were 2-1 for safety reasons.
“It was when I reflected upon the social and pragmatic presentations of ER that I began to draw upon my specialist training on the assessment and intervention of social communication disorders.”
Can you share some details on those assessments?
“I began by completing an assessment of self-awareness and self-esteem – Talkabout recommend that before even starting to work on social skills you must explore these first. If you have poor awareness of yourself and others, how can you have an accurate awareness of how you behave? Consequently, changing these behaviours will not be possible if insight is lacking.
“The assessment concluded that ER had poor awareness of both himself and others. For example, he was unable to describe his physical characteristics nor the qualities of those closest to him. An assessment of social skills was completed with the TDT, including body language, the way he talked, conversation skills and assertiveness. Unsurprisingly, significant deficits were found in the areas of distance, gesture, facial expressions and fidgeting.
“Following this I completed an assessment of emotional perception (The Awareness of Social Inference Test-Short). This revealed that ER was able to identify when people were generally happy or sad from their facial expressions, but he was unable to differentiate various types of negative emotions such as anger, boredom, anxiety or fear, known as alexithymia. This was a pivotal moment in understanding ER’s social behaviours and explained why ER demanded that people “smile” during any social interaction. ER could identify if people were looking unhappy but was unable to understand specifically why.
“The presence of social communication impairments posed a significant risk in daily interactions if ER’s intended communication was misinterpreted by others. This increased his level of vulnerability both from and towards others on the ward, in the community and when interacting with his family.”
Wow, that’s quite a key issue that you uncovered, how did you support ER once you’d realised this? What did this new understanding mean for ER’s rehabilitation in general?
“Having a clear understanding of ER’s impairments meant that we could support him to identify the key areas that he wanted to work on. We set four main rehabilitation goals:
- To demonstrate appropriate social distancing with a visual cue.
- To remain seated for 45 minutes during a therapy session.
- To greet people saying, “how are you?” rather than exclaiming “SMILE!”
- To reduce the scale of gestures with a visual cue.
“ER engaged in an initial block of therapy aiming to improve awareness of himself and others. Following this, intervention focused on distance, fidgeting, reading facial expressions and gestures. We also worked on identifying what different types of facial expressions mean in terms of how the person is feeling, and the most appropriate way to address them based on this. ER’s engagement with therapy had such a positive impact on the achievement of his goals. Reading facial expressions is still difficult for him, but instead of demanding “smile!” he asks, “how are you?” when unsure how people are feeling.
“Due to significant memory difficulties ER requires visual cues to make changes to his social communication behaviours. For example, if standing in close proximity he is prompted with an outstretched arm to measure the socially acceptable distance to stand. If he uses exaggerated greetings he is prompted by pointing discretely to your hand to reduce the scale of his gesture.
“ER continues to have active rehabilitation goals. We are working on generalising the gains that he has made in therapy sessions to other situations and environments. One objective is to take the drinks order of two other patients when they are having refreshments. Not only does that continue to improve his cognitive communication and memory skills, but it’s also being a positive role model to the other patients.”
That’s fantastic progress, and wonderful that he is becoming a positive role model for other patients.
“Yes absolutely – the improvements in his communication skills can also be seen in his interactions with other patients here at the Avalon Centre. For example, ER will now often sit and chat with a patient who has dementia, and would sometimes display challenging behaviours. There have been subtle changes in how this patient communicates with staff and peers, as he now initiates interactions and asks ‘how are you?’, modelling ER’s positive behaviours.
How has working with a TDT’s supported ER’s rehabilitation?
“Working within a transdisciplinary team means that there is ownership of rehabilitation goals across the therapy and nursing team. For example, ER had four main goals for his speech and language rehabilitation programme but these were also practised in other settings and were added to his Community Access Programme. This facilitated the generalisation of positive social communication interactions in meaningful and functional activities. So that means that whenever ER was in the community, in the supermarket doing his shopping, in the bowling alley, these goals continued. Speech and language therapy continued whenever he was interacting with occupational therapy, physiotherapy, psychology and even with his family.”
And have you seen improvements with ER because of this TDT approach?
“Yes absolutely. 1-1 SLT sessions paused for eight weeks in order to determine if ER’s gains in self-awareness, self-esteem and social skills would be maintained in the presence of the TDT model of neurobehavioural rehabilitation. During this time he continued to engage in the core group therapy timetable as well as other individual therapy disciplines. Upon reassessment I found that not only have his skills been maintained but they have further improved, demonstrating the power of the TDT approach in generalising impairment-based interventions into functional activities. This has had a significant impact on ER’s outcomes – ER is now being supported to visit his family in preparation for eventual discharge home.”
Assessment of Social Skills
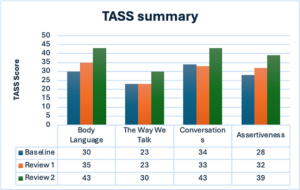
Baseline prior to intervention on self-awareness, self-esteem, and social skills – 20/11/2023
Review 1 post intervention – 29/02/2024
Review 2 following 8 week pause from direct 1-1 SLT intervention – 23/05/2024
References:
Mehrabian, A. (1971) Silent messages. California: Wadsworth.
Make An Enquiry
If you’d like to make a referral then please get in touch with us.
You can also visit each service’s profile page to find out more about what our EveryExpert approach to care looks like in practice:
Adderley Green, Staffordshire
Badby Park, Northamptonshire
Garden & Jacobs, Hertfordshire
St Neots, Cambridgeshire
Stanley House, Herefordshire
The Avalon Centre, Wiltshire
The Bridge, Middlesbrough, Wiltshire
The Dean, Gloucestershire
